Raising the bar for routine M&E in GBV programs – From recognition to diffusion


The International Rescue Committee (IRC) 2020 strategy is evidence based and outcome driven. The premise of the Gender-based Violence (GBV) response theory is that women and girls are safe and use quality services that treat physical, mental and social consequences and prevent any additional harm. The theory articulates what is required for services to be truly accessible to women and girls and what elements are necessary for services to be of good quality. The theory also acknowledges the barriers that most often prevent women and girls from seeking care and the necessary knowledge, attitudes, skills, and support they need to take the first step toward treatment and to seek and receive ongoing support for physical, mental and emotional injuries. Underlying this theory is a persistent social norm that women and girls are equally entitled to a complete state of well-being and that all forms of GBV are unacceptable. The systems that support health service delivery and psychosocial support services for survivors must be functional, well-coordinated and bolstered by a community norm that women and girls are as equally entitled to the pursuit of health and well-being as men and boys.
But how do implementers hold themselves accountable to all of the above when all we know by the end of the day is the # of dignity kits distributed, the # of survivors assisted and the # of staff trained? How do we improve quality and access across the continents during crises when resources are scarce the only way to reliably measure outcomes is through rigorous mixed method research?
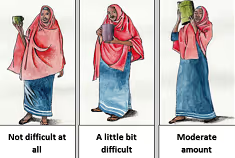
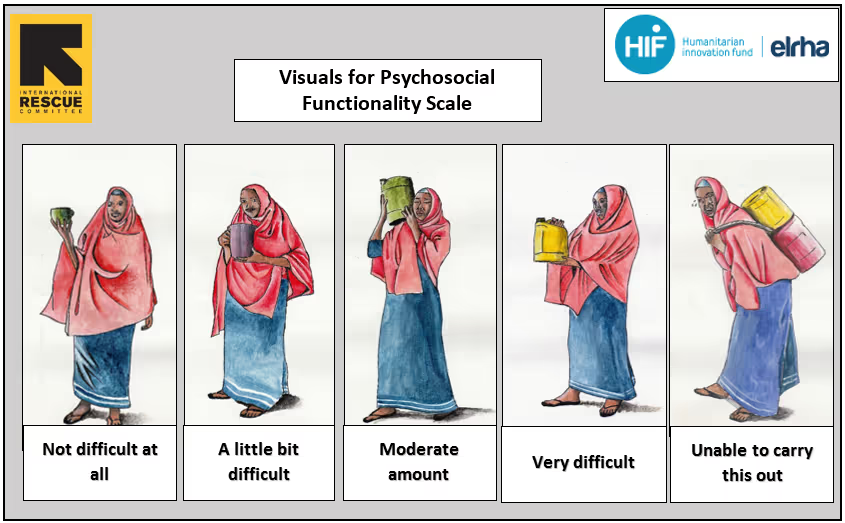
The IRC committed to finding a solution to the challenge by developing simple tools for measuring outcomes around ‘felt stigma’ and ‘psychosocial functioning’ among women and older adolescent girls receiving GBV case management. Though it has been a bumpy road, it has also been interesting and educating and we’re happy to present the new tested and validated tool kit which is currently adapted for Syrian refugees in Jordan and Somali refugees in Kenya. The tool kit is accompanied by guidelines for adaptation to other humanitarian and development contexts and populations. These resources are freely available at IRC’s GBVResponders.org.
What is so special about this tool? Well, during the innovation process we discovered that survivors preferred to take the survey during regular GBV case management and with a trusted (known) case worker. As a result, data will be collected as an integrated part of case management and the 10 item questionnaire will help the survivor and the case manager to identify progress or set-backs in the healing process. The two tools can either be used together or separately – and measure improvement over time or a snap-shot of the survivor’s state of functioning and/or felt stigma.
The IRC’s journey with the HIF started exactly 2 years ago at the ‘GBV measurement challenge’ workshop in London. We have now come to the end of the road for this project and we very much look forward to taking this to scale as well as finding new ways of measuring essential outcomes in GBV programming and low-income humanitarian settings. Our hopes and dreams for the newly developed GBV outcome measurement tools are, that they will inspire implementing partners, donors and UN agencies to shift the focus from output to outcomes. And possibly stimulate the GBV community to join us in further development of a new M&;E culture within GBV programming.
For any questions around the tool or its application, please contact [email protected] or [email protected]

Stay updated
Sign up for our newsletter to receive regular updates on resources, news, and insights like this. Don’t miss out on important information that can help you stay informed and engaged.





Explore Elrha
Learn more about our mission, the organisations we support, and the resources we provide to drive research and innovation in humanitarian response.